People
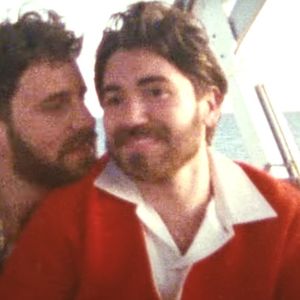
Kelsey Louie is The Metamorphosis Man

He's helping to transform the venerable GMHC from the inside out.
June 08 2016 4:00 AM EST
May 26 2023 2:41 PM EST
By continuing to use our site, you agree to our Private Policy and Terms of Use.
He's helping to transform the venerable GMHC from the inside out.
Photo courtesy of Chris Hayden Photography.
In activist circles, where long-term survivors offer a world weary but wise perspective as leaders, some still think of Kelsey Louie as the new kid on the block. Still baby faced at 41, the executive director of GMHC “was too young to have my peer group decimated by the epidemic. However, the generation right before me certainly was. A lot of my mentors and some colleagues and some friends certainly were impacted during that time in the ’80s. I just wanted to give back.”
Wanting to be of service, both to the LGBT world and to those impacted by HIV, Louie started as a child therapist and social worker (he has an MSW from NYU and an MBA from Columbia), focused on issues around substance abuse. That experience gave him an understanding of “the impact of substance abuse and mental health issues, related to HIV and AIDS.”
His first job in the HIV-world was as clinical coordinator at GMHC in 2006. He then spent seven years at Harlem United Community AIDS Center, where he “learned the importance that housing plays in the AIDS epidemic and how stable housing is critical.” He continued to move up at Harlem United, eventually becoming the chief operating officer before returning to GMHC, this time as chief executive officer.
Louie took over GMHC, New York City’s largest HIV service organization, after tumult threated to tear the organization apart. The board of directors had ousted former CEO Marjorie Hill, who reportedly had angered both staffers and clients with opaque decisions about money, pay cuts, and the group’s spacious new offices that critics argued squandered money. Hill’s departure was painted as a mutual decision, but it’s safe to say, at best, Louie walked into a situation with folks who were cautious all around him.
What he did next surprised some. He listened. And some say it was a long time coming.
“One of the things that I do at GMHC is that I listen,” Louie says. “I listen to the current clients, I listen to the staff, I listen to my mentors, I listen to long-term survivors. It’s proven to be very valuable to me to listen more and to listen before I take action.”
He had to start by rebuilding the relationships with both clients and overworked staff. “I wanted to make sure that the staff felt that they can be proud of working at GMHC. They have a lot of input into the decisions that I make,” he says.
He was also intent on making “sure that we are good stewards of public and private dollars and making sure that we’re making the most out of every dollar that we have.” One of his earliest decisions was to consolidate GMHC’s space, the offices that were such a point of contention. “We gave up the entire seventh floor and reduced our space by 25 percent, which reduced our rent by 25 percent.”
And he mended fences, something that paid off not just in PR and goodwill but on his own professional bucket list.
“One of the most exciting things that I have done in my entire career — and life — is to re-engage Larry Kramer back into the arms of GMHC,” says Louie. “And how powerful and meaningful it was for him to receive that embrace and to openly and publicly call GMHC his first child. And for him to push me to make sure that GMHC is being loud in the areas that we need to be and for others to be [quiet]. It’s a lot to live up to.”
Kramer, who co-founded what was then called Gay Men’s Health Crisis in 1983, was later booted from the organization because of his brash and often controversial methods of raising awareness about the AIDS epidemic. His story was loosely translated into The Normal Heart, which became a blockbuster film in 2014 starring Mark Ruffalo and Julia Roberts.
Over 30 years later, Louie welcomed Kramer back into the fold at GMHC last year, and recently honored Kramer and another surviving founder, Dr. Larry Mass, telling the crowd that the two founders’ “refusal to accept political paralysis and the early public apathy toward the AIDS plague truly changed the world.”
“Without Larry Kramer and our founders, there would be no GMHC,” Kelsey later told The Advocate. The founders’ “activism, their relentlessness in the face of a terrifying, unknown disease saved countless lives. Mr. Kramer’s impact is very hard to measure, because it’s so profound and so far-reaching.”
Louie himself wants to have a similar impact and he’s brought about some sweeping changes at GMHC to do so. Some symbolic, others substantive, together they make it clear that Louie is determined to stop at nothing short of metamorphosis with New York’s largest HIV service organization.
He’s proud that after just two years, “almost all of our processes are [now] transparent,” a bold decision for an organization long charged with being secretive.
He’s investing in GMAC’s staff with a new job training program, and doubling down with some heavy-duty partnerships, including some that demonstrate what Louie sees as the intersectional issues at the core of GMHC’s mission. The organization played a significant role in New York’s Blueprint to End the AIDS Epidemic by 2020. What started as a governor’s task force became a 63-person coalition that detailed the efforts needed to reach that goal. It’s a simple plan on paper: identify everyone with HIV, get them into care, and get their viral load suppressed so they can’t transmit HIV to others; while simultaneously getting people at risk for HIV on PrEP so they stay HIV-negative. But the task ahead is staggering: reduce the number of new HIV infections to just 750 (from an estimated 3,000) by 2020 and achieve the first ever decrease in HIV prevalence in New York State.
“What came after [the blueprint] is the real, actual work,” says Louie. “What we did is we partnered with other organizations to really attack certain recommendations from that blueprint. For example, we worked with SAGE to work with the older adults and long-term survivors. We have a bunch of strategic initiatives that we turned into action plans rather than things that will sit on a shelf.”
GMHC engaged on a federal level too, working with the White House to develop “the National HIV/AIDS Strategy updated to 2020. We’re really strategizing and really capitalizing on all of our resources,” he says. And he says, we can’t forget GMHC’s “not so obvious partners…like Planned Parenthood. We stood in support of Planned Parenthood because they provide hundreds, if not thousands, of HIV tests every year.”
There were also “three simple but meaningful changes” to their logo, a reflection of where and who they are now. “First we changed the color from magenta to red, honoring our past — we wanted to go back to the traditional color of HIV and AIDS. Second, we changed the words ‘Fight AIDS’ to ‘End AIDS.’ And we changed the phrase ‘Love Life’ to ‘Live Life’ because all of our services are geared towards helping people live full and rewarding lives, regardless of their HIV status.”
Those may seem small and symbolic, but even clients tell us they’re seeing changes afoot. For many, it’s about knowing they have Louie and his staff’s attention, something many say is happening more now than ever.
He’s not only talked to, but has been moved by conversations with long-term survivors who felt forgotten, and with trans people who share similar concerns. One trans client begged Kelsey, “Louie, please use your privilege to help us. Based on the numbers of people who are dying — we are facing our own epidemic.” Indeed, as 60 percent of trans women of color are HIV-positive, there’s an urgent need there. “When you look at the data,” Louie says, “the transgender population is disproportionately impacted by HIV. To know that we could be doing more for them, for our trans brothers and sisters is so critical to what we do. We won’t end the epidemic unless we address this population as well.”
Louie feels a particular debt to long-term survivors, the gay and bi men who really formed the GMHC community decades ago.
“With the long term survivors, to think that GMHC was no longer meeting the needs of a particular group that we were built to serve, really impacted me,” he admits. “So much that I knew that we needed to do something.” In response the organization enhanced their programs for long-term survivors and re-launched their Buddy Program, which was one of GMHC’s earliest services.
Both of those conversations impacted Louie greatly, and in turn impacted the services and leadership GMHC has pursued.
The group has been a leader on PrEP education in New York, hosting workshops and science-driven panels for gay and bi men, trans women, and other folks who are most at-risk.
“We have a tool that can prevent HIV infection,” Louie says. “Could you imagine what would have happened if we had a pill that could prevent HIV in the ’80s? I’m alarmed at the low uptake of PrEP.”
The group’s biggest change yet is still in the works, but it’s a critical part of GMHC’s strategic plan going forward.
“When I first got here… clients [weren’t] really engaged or receiving integrated care. Only 10 percent of our clients were receiving more than one service. Most people were coming in for a hot meal and leaving [or] coming in for a legal services and leaving. We all know that disjointed and uncoordinated care is not as effective as integrated care. We realigned all of our programs to make it easier for staff and clients to understand what we were doing and what we offered. We’re excited to say that right now about 30 percent of our clients receive more than one service. We’re doing more to coordinate their care.”
Next up, the organization is going to secure a mental health and substance use license so they’ll be able to expand those services.
“More importantly, or larger, is we have decided to pursue health care. Over the last 30-plus years, GMHC has been a cornerstone of HIV/AIDS care, prevention, and support. In order to really move us past the finish line and end this epidemic, we believe that we need to offer medical services.”
Louie boasts “that of the people that test positive at our testing center, 90 percent of them become virally suppressed, because of the model that we use to connect people to medical care. It’s that 10 percent that continue to drive the epidemic. We believe that if we can offer our own health care we can capture some of that 10 percent. If we offer healthcare, we might be able to connect even more people to healthcare. So, that is our vision for the next few years — to pursue our own medical license.”
That all takes money, of course. “In recent years we’ve been saying, ‘We have the data, and we have the tools — all we need is the political will.’ We’re not there fully because right after political will comes dollars. We need the dollars …[for] programs and health care and access to medication. But we also need to address the secondary drivers of the epidemic: stable housing, mental health, mental illness and substance abuse issues, stigma, racism.”
The leader’s speech at GMHC’s spring gala touched on those issues, too, using translation as the key: “Sometimes translation is required to ensure the same meaning for all,” he said. “Translating science into policy is required when irreversible disease progression is an absurd prerequisite to house a homeless person living with HIV. Translating statistics into action is required when the same inequities in access to treatment are repeated again and again in access to PrEP, for black men who sex with men, and high risk women. Translating statistics into action is required when 25 percent of all Latino MSM, and 50 percent of all black MSM are projected to contract HIV during their lifetime. Translating statistics into action is required when Trans women of color are disproportionately impacted by HIV…Translating headlines into real resources is required when flashy press events, hosted by politicians, do not yield the budgeted dollars promised.”
Sometimes it’s not about politics or policy, he admits. What he’s fighting is simply the stigma of HIV, of seroconversion itself, and even people with HIV’s own feelings about being poz.
“A lot of people don’t think it’s a problem anymore, or not as big as a problem. [Because of] stigma that’s related to it, people don’t talk about it. When people don’t talk about it or are afraid to talk about it, they certainly won’t get tested, they certainly won’t go to health care, and they certainly won’t stay in treatment.”
There’s positive change, but, he says, “Stigma has come a long way in becoming a big, bold cap issue for most HIV service organizations. Now what does that mean? You can’t attack stigma [just] one way because it comes in multiple forms. I talk to a lot of HIV positive people who whenever I talk to them I’m like, ‘Your biggest problem is your internal stigma. You are judging yourself before you even utter the words; you can’t even get out the gate because you haven’t actually experienced any real encounter that would make you feel this way but you’ve assumed yourself into a hole.’”
Want more breaking equality news & trending entertainment stories?
Check out our NEW 24/7 streaming service: the Advocate Channel!
Download the Advocate Channel App for your mobile phone and your favorite streaming device!