Stigma
Why Do Black Gay and Bi Men in the South Still Have Such High HIV Rates?

African Americans in the south never got a pepfar.
June 16 2017 7:44 PM EST
May 26 2023 2:56 PM EST

Increased funding, targeted prevention efforts and better treatment have helped to slow down the HIV epidemic in the United States. As the Centers for Disease Control and Prevention shows, the number of new HIV-positive cases has decreased significantly and the number of new HIV diagnoses declined by 19 percent from 2005 to 2014.
But this is not the case in many parts of the country. As AIDS and public health researchers, we are among those who are alarmed by areas in the southern United States where the number of cases have not declined, and even more, by areas that have actually increased.
We have seen disturbing trends in Prince George's County, Maryland, where we do research on AIDS and health disparities. These are similar to trends in other nonurban settings in the southern United States where a majority of African-Americans live.
According to the New York Times, "Last year, the Centers for Disease Control and Prevention, using the first comprehensive national estimates of lifetime risk of H.I.V. for several key populations, predicted that if current rates continue, one in two African-American gay and bisexual men will be infected with the virus. That compares with a lifetime risk of one in 99 for all Americans and one in 11 for white gay and bisexual men. To offer more perspective: Swaziland, a tiny African nation, has the world’s highest rate of H.I.V., at 28.8 percent of the population. If gay and bisexual African-American men made up a country, its rate would surpass that of this impoverished African nation — and all other nations."
The article goes on to say the crisis is most acute in Southern states, which hold 37 percent of the country’s population, and as of 2014 accounted for 54 percent of all new H.I.V. diagnoses. The South is also home to 21 of the 25 metropolitan areas with the highest H.I.V. prevalence among gay and bisexual men.
Jackson, the capital of Mississippi (the country’s poorest state) is best known for blues, barbecue and The Help. It also has the nation’s highest rate — 40 percent — of gay and bisexual men living with H.I.V., followed by Columbia, S.C.; El Paso, Texas; Augusta, Ga.; and Baton Rouge, La. In Jackson, a small city of just over 170,000, half a dozen black gay or bisexual men receive the shock of a diagnosis every month, and more than 3,600 people, the majority of them black men, live with the virus.
The South also has the highest numbers of people living with H.I.V. who don’t know they are positive, which means they are not engaged in lifesaving treatment and care and are at risk of transmitting it to others. An unconscionable number of them are dying: In 2014, according to a new analysis from Duke University, 2,952 people in the Deep South died with HIV. as an underlying cause, with the highest death rates in Mississippi and Louisiana. Among black men in this region, the HIV-related death rate was seven times as high as that of the United States population at large.
Southern nonurban black communities in crisis
In Prince George's County, Maryland, a suburb of Washington, D.C., the number of new HIV infections has increased from 2014 to 2015, according to the Maryland Department of Health and Mental Hygiene. In fact, Prince George's County leads the state in the number of new HIV diagnoses, having surpassed Baltimore City in 2013.
With rates that are 20 times higher than those of whites in 2015, African-Americans are disproportionately impacted by HIV in Prince George's County. In 2015, African-Americans constituted 86 percent of all new HIV diagnoses and 85 percent of the total population living with HIV.
Moreover, engagement in HIV care remains at critically low levels among those living in Prince George's County. Only 49 percent of people living with HIV are retained in care and 37 percent have achieved viral suppression, when a person's HIV viral load is undetectable or is very low, considerably reducing the risk of transmission.
This public health crisis in Prince George's County reflects a much broader trend in the United States, where the disproportionate burden of HIV is increasingly found in the U.S. South, including Washington, D.C., Maryland, North Carolina, Georgia, Florida, Mississippi, Louisiana and Texas. In many areas, HIV is concentrated in urban areas.
But in the South, larger proportions of those diagnosed with HIV are living in smaller metropolitan, suburban and rural areas and places like Baton Rouge, Louisiana; Jackson, Mississippi; Memphis, Tennessee; Columbia, South Carolina; and Lowndes County, Alabama.
Southern states have the highest rates of new HIV-positive diagnoses, the highest percentage of people living with HIV and the lowest rates of survival for those who are HIV-positive. Nearly 52 percent of all new diagnoses of HIV in 2015 occurred in southern states, even though only 37 percent of the U.S. population lives in the South.
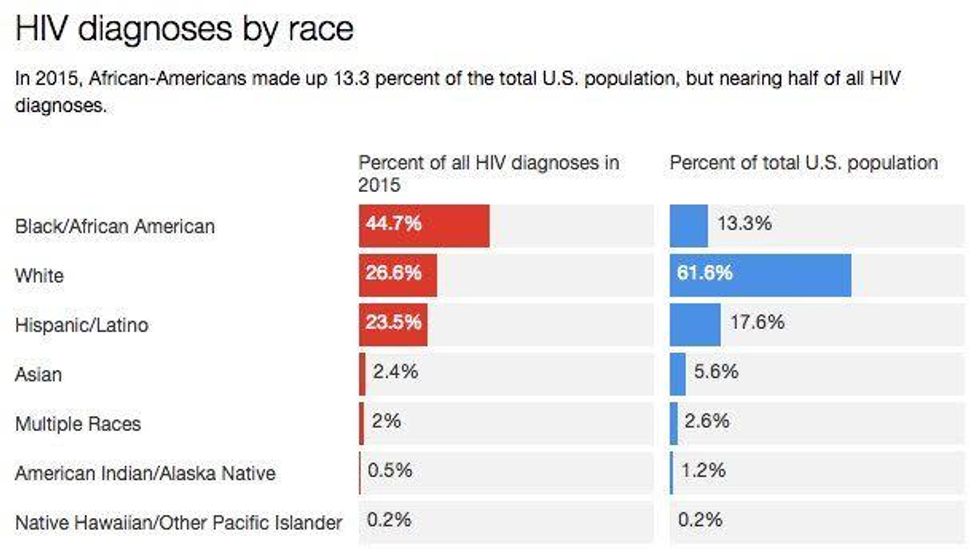
The vast majority of African-Americans live in the South, and they are the hardest hit by the HIV epidemic in the region.
In 2015, African-Americans accounted for 45 percent of HIV diagnoses in the United States overall, though they comprise 13 percent of the total population. But in the South, this percentage is much higher, with African-Americans accounting for 54 percent of new HIV diagnoses in 2014.
Black men who have sex with men have a disproportionate burden of disease, accounting for 59 percent of all HIV diagnoses among African-Americans in the South. Black women also face an unequal burden, comprising 69 percent of all HIV diagnoses among women in the South. Black transgender communities in the South are also heavily impacted. Half of all transgender persons who are diagnosed with HIV are black. Around half of transgender people who received an HIV diagnosis between 2009-2014 lived in the South.
Root causes of the enduring HIV epidemic in the South
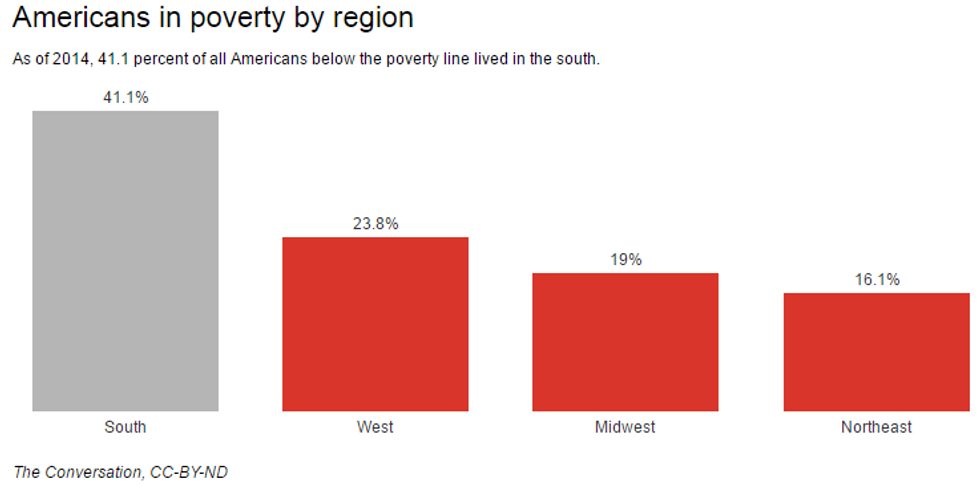
The South suffers from disproportionate rates of concentrated poverty and the clustering of poor populations in very poor communities. That increasingly exists in smaller cities, suburban areas and rural counties.
In 2010, 41 percent of poor Americans lived in the South, according to the Pew Research Center. Research has shown that in these areas of concentrated poverty, poor families are saddled with additional burdens, beyond what the families own individual circumstances would dictate, including inadequate access to quality health care and poor health outcomes.
Abstinence-based sex education and criminalization of HIV-related risk behaviors, rooted in perceptions that HIV is associated with immoral and deviant behavior, has resulted in increased stigma and discrimination toward those living with HIV in the South. This can lead to people being afraid to get tested or seek treatment for fear that someone may find out they have HIV.
Stigma and discrimination are also found in many middle-class and wealthy African-American communities in the South, like those in Prince George's County, where black respectability politics and the notion that by adopting certain cultural norms of the white mainstream, black people can protect themselves from discrimination and has contributed to a silencing of the HIV epidemic among the African-American poor and the blaming of victims for their illness.
Finally, health care and funding disparities have long plagued the South and have contributed to the rising rates of HIV in the region. Federal government funding still lags behind for southern states. For example, 33 percent of federal funding was distributed to the South, despite the region having 52 percent of all new HIV diagnoses in the country.
The CDC has increased funding to the South to directly reflect the impact of HIV in the region, with an increase of 22 percent or US$36 million from 2010 to 2015. However, many community-based organizations doing frontline HIV prevention work are ineligible for funding because they are not located within major metropolitan centers. The most recent CDC funding announcement for community-based organizations, for instance, focuses on people at high risk of contracting HIV only in metropolitan areas hit hardest by HIV and AIDS.
Additionally, southern states also have some of the strictest eligibility requirements and least expansive Medicaid programs. Many southern states rejected Medicaid expansion under the Affordable Care Act, which extended health care to millions of uninsured Americans. Such health care policies, along with poor health care infrastructure, lack of qualified health professionals and geographic isolation, have resulted in substandard or nonexistent health services and treatment for those most in need.
The proposed American Health Care Act will further limit the expansion of Medicaid, which would disproportionately affect the poor and may not provide insurance for those with preexisting conditions, including HIV.
Transformative actions need to occur in order to make a positive impact on the devastating effects HIV has had among African-Americans in the South. Funding needs to be reallocated to the region, especially to frontline providers and organizations doing HIV prevention work. Political pressure to expand Medicaid and to increase funding for HIV prevention and treatment is necessary to stem the tide of the epidemic.
People should advocate to change laws and policies, particularly around sex education and criminalization of HIV-related behaviors. Increasing opportunities for employment, housing and education can also improve HIV prevention in the South.
In order to make progress, southern states must make difficult structural changes such as increasing funding, health care access and treatment. They also need to directly confront the inadequate living and working conditions that put poor African-American youth and adults at heightened risk for HIV.
It also raises the question: why did'nt citizens of the United States, ever get their own version of President’s Emergency Plan for AIDS Relief (PEPFAR)?
Thurka Sangaramoorthy is Professor of Anthropology, University of Maryland and Joseph B. Richardson is Professor of African American studies, University of Maryland.![]()