Treatment
This Article Could Save Your Life

But only if the right person reads it.
August 24 2017 7:00 AM EST
May 26 2023 3:39 PM EST

In 2015, Joe Williams,* a gay man from Mississippi, experienced HIV-related renal failure. As his kidneys shut down, his ankles and feet became swollen and painful. Still, it was the extreme fatigue that really got him down. He’s in his 30s.
Williams promised himself a long time ago never to let HIV run his life, but it became increasingly difficult for him to pursue his dream of becoming an educator. He’d go to classes for his teaching credentials in between dialysis treatments, but it was a constant struggle. And, like many living with HIV, he wasn’t doing well on dialysis.
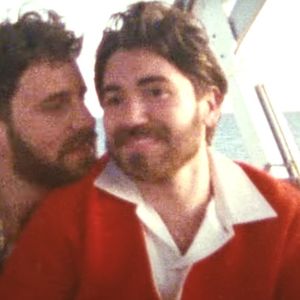
New Yorker Ken Teasley (right), a gay man from the Bronx, also ended up on dialysis. Teasley was a typical healthy high school student, who “drove a school bus and had a second job, ran long distance track, co-editor of my school newspaper, played cello — you know, normal stuff,” he says, sounding more accomplished than most teens.
Teasley was diagnosed with high blood pressure at 17, but still managed to pass an Army physical two years later. He moved to New York after getting out of the military and did what gay men are supposed to, he says, by getting tested for HIV “every six months until my first relationship.”
Teasley was 27 when he learned he was not only HIV-positive, but “only had 23 percent kidney function and, at some point, would require dialysis.” To prolong the inevitable, he made numerous lifestyle changes to lower his blood pressure and stop taking pain medication for the gout he experienced as a side effect of the kidney failure.
“I finally got off blood pressue meds, but the damage was already done,” Teasley says. In 2002, a doctor recommended he check out The Mount Sinai Hospital’s organ transplant program. It was one of only a handful of medical centers in the U.S. doing transplants into HIV-positive patients. But Teasley wasn’t ready.
“I didn’t want a transplant,” he admits, “until I started dialysis.”
HIV-positive individuals “on dialysis are twice as likely to die as compared to their [HIV-negative] counterparts,” says Dr. Shikha Mehta, medical director of the University of Alabama Birmingham’s HIV Transplant Program. “Research has shown that kidney transplantation reduces this risk of death by 80 percent as compared to staying on dialysis.”
Neither Williams’s nor Teasley’s living relatives were found to be matches, so they were each placed on the organ transplant waiting list. While Teasley was told he might have to wait seven or eight years before getting a donated kidney, Williams’s type O blood would make finding a match even more difficult. He might have to wait up to a decade for a kidney — if he lived that long.
 HAPPY DAYS: Kenneth Teasley (above), the first recipient of an HIV-positive organ transplant at The Mount Sinai Hospital.
HAPPY DAYS: Kenneth Teasley (above), the first recipient of an HIV-positive organ transplant at The Mount Sinai Hospital.
“There continues to be a supply and demand problem where we have more people in need of a kidney than we have kidneys available,” acknowledges Dr. Jayme Locke, surgical director of UAB’s HIV Transplant Program, where Williams’s transplant was performed. That’s why HIV-positive people continue to die waiting for kidneys.
According to HIV.gov, up to 30 percent of those living with HIV suffer from abnormal kidney function issues, which, left untreated, could turn deadly. While the disease itself can cause kidney damage, those on treatment are more at risk of nephrotoxicity, which is “toxicity or injury to the kidneys.” It can be a side effect of some HIV meds, including protease inhibitors and nucleoside reverse transcriptase inhibitors. Long-term survivors are particularly susceptible to this kind of kidney damage because of the length of time they’ve been on antiretroviral meds.
In addition, a number of comorbidities common in those living with HIV also increase the risks of kidney damage, including high blood pressure (which HIV-positive people are three times more likely to develop), diabetes (which poz folks are four times more likely to develop), and hepatitis C (which approximately one out of every four people with HIV also have). Poz people suffering from these other diseases further add to the number who experience renal failure, have issues on dialysis, and spend their remaining years on a transplant waiting list.
Mary Smith* was already aware she might need a transplant at some point when she discovered she had gotten HIV from her husband. “When I became HIV-positive, I was, ‘Oh god, what about if I need a transplant?’ I’m going back to 1990,” Smith recalls. “That always scared me, that I would never be able to get a transplant, because, at the time, no one even thought about it.” Indeed, since the height of the AIDS epidemic in the 1980s, HIV-positive individuals have been legally prohibited from donating organs, and doctors have been prohibited from transplanting HIV-positive organs into another person — regardless of the recipient’s status.
Because of the way HIV can attack the immune system, people living with the virus were once considered too high risk to even receive organ transplants. But in the 1990s, the federal government granted a few research facilities the opportunity to study the impact of organ transplants on people living with HIV. Dr. Sander Florman, director of Mount Sinai’s Recanati/Miller Transplantation Institute, says his hospital was one of the first “committed to the transplantation of people with HIV since way before it was ever anywhere near popular. I think the first HIV-positive transplant was done in 1998 here. And that was at a different time when people were very scared of HIV.”
Florman explains further: “Mount Sinai found many of our anti-rejection medicines actually work synergistically with the HIV medicines to prevent the virus. And that’s part of the secret to why people with HIV can have successful organ transplants, which was heresy 10 years ago.”
Alabama-based Locke has also conducted research showing that HIV-positive individuals who receive kidney transplants can have “excellent long-term outcomes.” Locke says her subsequent study that came out last year “also demonstrated a significant survival benefit.”
“No one had ever really shown that,” Locke explains. “They’d shown good outcomes after transplant, but no one had ever been able to quantify the survival benefit that an HIV-positive person receives by getting a kidney versus waiting on dialysis. We were able to demonstrate that as well, providing even more evidence that this is the right thing to do for this vulnerable population.”
In 2012, Teasley was feeling particularly vulnerable himself when he was diagnosed with kidney cancer.
“My mother, sister, and I were [all] diagnosed with cancer within six months of each other,” he recalls. That’s when Teasley discovered that having a cancer diagnosis made him “inactive” on the organ transplant list.
Teasley eventually had his cancerous left kidney removed and says his family all survived and all three remain cancer-free today. Still, he was told post-surgery he’d have to wait an additional two years before his transplant listing was active again. He was looking at 2019 or 2020 before a kidney would become available.
Things weren’t looking good for Smith, either. The polycystic kidney disease she’s had since 1986 had “just gotten worse” over the decades. One of the hurdles Smith faced was financial. She’s on Social Security disability, but to get Medicaid insurance coverage, she’d have to pay. Not wanting to spend any of her meager income, Smith put it off until last year. But she “was getting weaker and sicker,” so she decided it was time to try for a transplant, and to do so she “had to pay six months up front in order for them to start the ball going. That’s how I ended up on the regular list; I got moved up to be officially on the list.”
After that Smith says, “My daughter and my sister both tried to be organ donors for me, but we didn’t match. Then I realized I could do a swap. So, my daughter is in the process of that.”
A swap (or chain) happens when a donor isn’t a match for their planned recipient.

 SAVING LIVES: The transplant team in the operating room at Mount Sinai with surgeon Sander S. Florman (bottom, right).
SAVING LIVES: The transplant team in the operating room at Mount Sinai with surgeon Sander S. Florman (bottom, right).
“About half of the people who come forward to be living donors are going to be found not matched with their intended recipient,” explains Locke, whose lab has the “longest” kidney chain in history. “What a chain does, it takes an individual who wants to be a living kidney donor but doesn’t know anybody who needs a kidney. They are matched to a person who has a donor, but their donor doesn’t match them. So that altruistic donor gives to that recipient, then that recipient’s original donor gives to the next incompatible pair, and so on. It’s like a domino reaction. It creates a bunch of compatible transplants that otherwise would not have occurred.”
Having a donor willing to donate can certainly speed up the chances of you getting an organ, but still, the wait can drag on. And, especially for people with HIV, waiting can be deadly.
That’s why after years of lobbying by the United Network for Organ Sharing, HIV activists were thrilled when the federal government finally reversed their policy with 2013’s HIV Organ Policy Equity Act. The HOPE Act, which went into effect in late 2015, authorized the use of organs from HIV-positive donors for transplantation into HIV-positive recipients.
“I found out about the HOPE Act, which I think is fabulous!” Smith says. “I don’t know why it took so long, you know, when so many people could’ve been saved. So, I said, ‘Well, go ahead and put me on that [list], too!’”
Doctors believe those who are already HIV-positive can safely receive organs from another poz person, and in doing so, free up organs for those who aren’t HIV-positive. “So, it’s a net gain for the system,” Locke says.
“To my surprise,” Teasley recalls, in 2016, “I was asked to participate in this new protocol involving an HIV-positive transplant.” Last summer, just two months after signing the paperwork, Teasley became one of the first people to receive a kidney from an HIV-positive donor. “I still have to pinch myself,” Teasley says. “My health is back on track. And by back on track,” he jokes, “I mean, I developed diabetes at two months post-transplant because of the steroids [given to prevent organ rejection].”
Florman performed Teasley’s historic transplant surgery, which was “the first time that we’ve been legally allowed to use HIV-positive organs” at Mount Sinai. Even in the best of situations, getting an organ can take years. “There are over 90,000 people listed that are waiting for a kidney transplant,” Florman says. “And there are 58 organ procurement organizations, and yet only a small handful have produced HIV-positive organs.”
The HOPE Act also included the caveat that transplants only occur “under approved research protocols designed to evaluate the feasibility, effectiveness, and safety of such organ transplants.”
Florman says that’s a smart move because, “We don’t know the answer to what will happen when we give an HIV-positive patient an organ from somebody with HIV. Could there be another strain of
the virus that overtakes their strain? What
if we gave them an organ with a strain
of HIV that wasn’t able to be controlled? Could we potentially make their HIV worse
and even… trigger something that would lead to AIDS?”
These are the questions that concern Smith too. “I have my HIV under control,” she says. “Murphy’s law: [what if] I catch a disease that I can’t treat?”
Whether that’s possible still isn’t clear.
“There’s no guarantee that when you transplant you would transmit HIV,” says Florman. “You’re not getting blood, you’re getting a kidney that has been washed out with our preservative solution. We do have some loose data from some older studies that show there probably is detectable virus in the kidney itself, but whether or not that would transmit [HIV], into the recipient is not clearly known.”
Researchers want to assess these concerns before making transplant surgeries widely available.
One discovery Florman made after completing just eight kidney transplants was a pleasant surprise for both surgeon and organ recipients: “Half of those kidneys have been in people where the test was a false positive,” which means the donor wasn’t actually HIV-positive at all, and 50 percent of Florman’s transplant patients received healthy kidneys. “The screening test for HIV in donors is not very sensitive,” he explains. “As a screening test, you want it not to miss any cases. Those organs, by law, prior to the HOPE Act… had to be discarded. We weren’t legally allowed to procure them. But now that we have the HOPE Act, we can still offer those organs only to people with HIV.”
Unfortunately, for all the insight the HOPE Act’s research caveat may provide, it also limits the number of facilities authorized to undertake such transplants. The United Network for Organ Sharing reports 13 hospitals have enrolled with the Organ Procurement Transplantation Network to participate in research studies.
“Only a dozen programs or so have agreed to transplant these organs,” Florman confirms. “And only two or three programs that have actually transplanted these organs, when there are 250 or 300 transplant programs out there.”
State laws also hamper the pace of adoption, so activists like Rick Zbur of Equality California have pushed for laws authorizing the surgeries (California’s Governor Brown signed such a bill in 2016).
Florman says another barrier is the fear surgeons have of acquiring HIV. Although the fear is overblown, Florman does acknowledge there is risk to the surgeons doing the procurement. “These organs don’t just appear,” he explains. “We have to go to other hospitals… we’re flying off to other parts of the country… [having] to go actually operate in another hospital with a team [we]’re not used to.”
Worse, deceased donors can’t share their medical histories (like which strain of HIV they have and if they are resistant to drugs) and may have been diagnosed as HIV-positive for the first time when they were brought in to the hospital. “We don’t know their history… or even if we do, they often may have viral loads that are detectable,” which is different from the recipients — who must have their HIV suppressed to undetectable levels before the procedure can proceed.
Floorman says, “because the organ procurement agencies share these same type of sentiments,” few have begun accepting HIV-positive organs even though it’s now legal for HIV-positive folks to donate. “I don’t think they mean any ill will,” he adds. “I think there’s [just] a lot of fear.”
In the first 12 months after the federal law went into effect, facilities like Mount Sinai and UAB performed 19 transplants (13 kidney and six liver transplants — some to the same recipient). At least 80 people living with HIV signed onto the waiting list for poz organs the first year, providing a sense of how much need currently outpaces supply. Even if donor matches were immediately found and made available at the speed of current HIV-positive transplant surgeries, it could take another four years to get all 80 off of dialysis. When every year could be your last, four can seem like a lifetime. There are simply not enough HIV-positive donors to go around.
Although Smith is still waiting, Williams was one of the lucky ones. He was matched with a donor and became the eighth person in the U.S. to receive a poz kidney, through UAB. “The very disease most people consider a death sentence is the same disease that has now given me a second chance at life,” Williams said several weeks after the surgery. “I am truly grateful.”
Teasley is more than thrilled to have received a kidney. “I get to keep my promise to myself to serve the community,” he says. “What better way to serve my community and other communities of color than to help provide much needed data to help future generations bridge the disparity gap, dispel some stigmas, and to provide hope to those afflicted around the globe? All the research that I and my fellow HOPE transplantees provide can potentially help countless people all over the globe.”
Locke hopes to get the word out to people living with HIV that
they can now be organ donors. “They can be a part of the solution,” she says. “HIV-positive individuals can give back to other HIV-positive individuals.”
Smith doesn’t care who donates her organ. “I don’t look at it as whose [organ], just something that’s healthy [so] I can feel normal again.”
*Name changed for privacy, upon request.