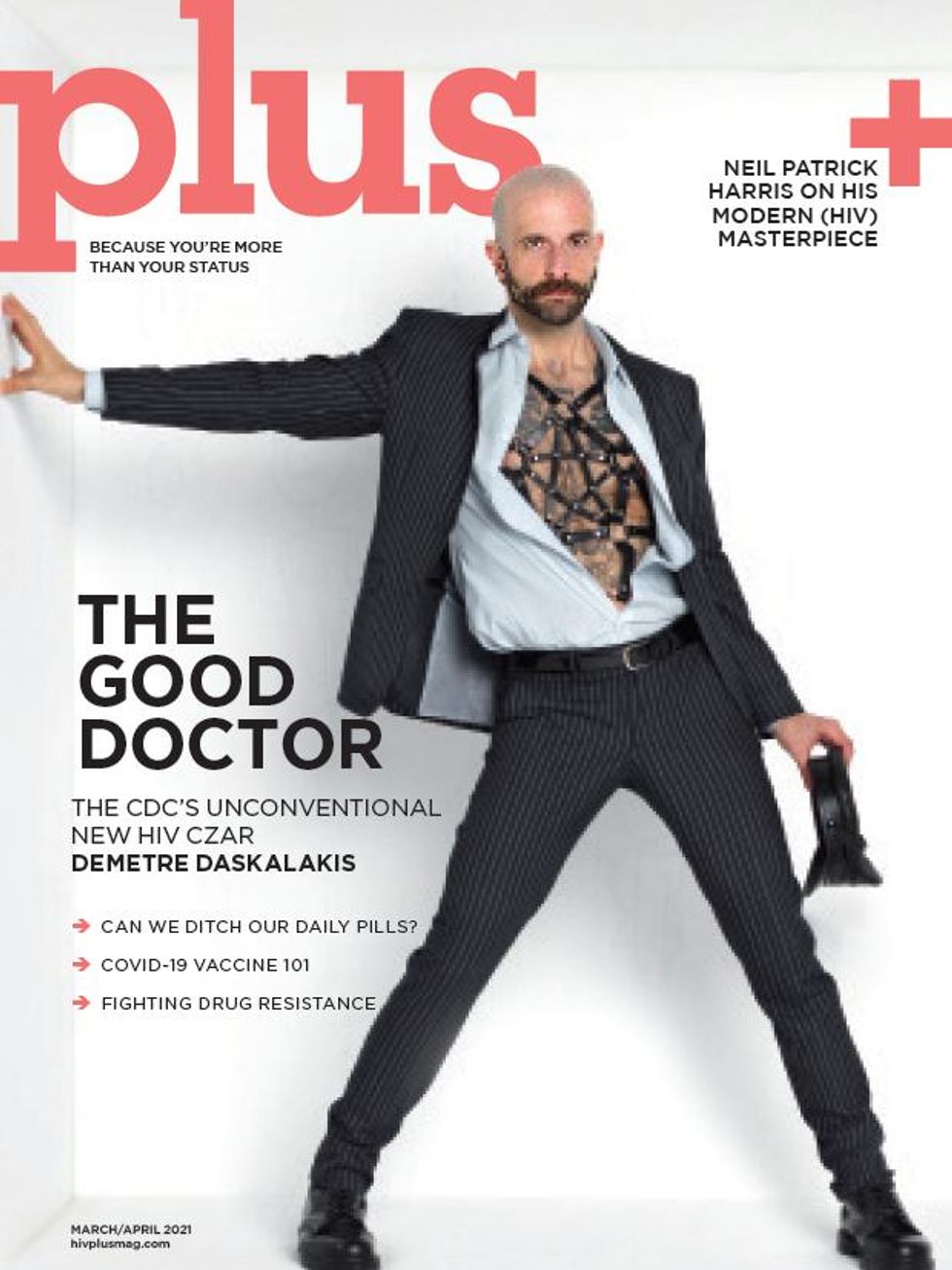
If Dr. Demetre Daskalakis is harboring anxieties over taking a new national health position in the middle of two global pandemics, it doesn’t show.
Formerly the deputy commissioner for the Division of Disease Control at the New York City Department of Health and Mental Hygiene, Daskalakis was hired as director of the Division of HIV/AIDS Prevention at the Centers for Disease Control and Prevention late last year. His first weeks on the job coincided with a frightening transition of presidential leadership, an insurrection at the U.S. Capitol, and devastating numbers of COVID deaths in the nation — typically between 2,000 and 4,000 fatalities a day.
But Daskalakis, one of the most visible government officials overseeing HIV policy, does not sound panicked or overwhelmed in a recent conversation with Plus.
“It’s a great time to land,” Daskalakis says. “We’re at a crossroads of strategy and implementation. Leading CDC’s Division of HIV/AIDS Prevention is my dream job. I believe that everything I’ve done in my career has been leading me to this role.”
Daskalakis is indeed perfect for the job of overseeing HIV prevention efforts at the CDC, officials from the government agency noted when announcing his hiring. Daskalakis was central in leading many HIV and STD programs in the nation’s largest city, including the Ending the Epidemic program, credited with bringing HIV cases to historic lows.
The gay doctor is known as an “activist physician” to some, as he’s been happy to serve as a public advocate for people with or at risk of sexually transmitted infections — giving interviews, attending fundraisers, dressing in drag to administer meningitis vaccines, and participating in public service announcements about the importance of treatment and prevention (one of Daskalakis’s stigma-battling efforts included a mid-2010s HIV web series he hosted on Plus’s website, The T With Dr. D).
Daskalakis was always more than a public face or figurehead, though. Raised in Virginia and trained in prestigious New York and Boston hospitals, Daskalakis was an attending physician at the Big Apple’s Bellevue Hospital and medical director for the city’s nationally respected Mount Sinai Health System before being hired in 2014 as assistant commissioner of disease control for New York’s Department of Health. At that time, the doctor saw a huge opportunity with the Affordable Care Act and the expansion of health insurance, especially among many young people. Daskalakis aggressively promoted PrEP (pre-exposure prophylaxis) for those at risk of HIV and TasP (treatment as prevention) for those living with it.
As part of his TasP efforts, Daskalakis spearheaded an effort known as “status-neutral care,” which aims to treat all patients the same, regardless of HIV status. That approach includes testing all patients unaware of their HIV status and then offering follow-up care, regardless of the test’s results. The goal is to keep as many people as possible either HIV-negative or unable to transmit the virus if they are HIV-positive by getting those individuals immediately on treatment. Not only does the method expedite care and prevention, but it also tackles stigma by treating everyone the same and not assuming anyone is specifically susceptible to HIV.
Between 2013 — shortly before Daskalakis joined the NYC Department of Health — and 2017, the rate of new HIV infections in the city among gay and bisexual men dropped by approximately 35 percent.
Now many look to Daskalakis to replicate his efforts on a national level, during a time when the COVID-19 pandemic is exacerbating physical and mental stresses for everyone on the planet, including people living with HIV. The CDC’s new not-so-secret weapon connected with Plus to share his plans moving forward.

Congratulations on your new position at the CDC. Did you have second thoughts about taking on such an important role amid the COVID pandemic?
I am very excited about this opportunity.… [The] CDC leads HIV prevention efforts in the U.S. and is playing a key role in the Ending the HIV Epidemic initiative. This federal initiative builds on the work CDC has been doing and aims to accelerate the reduction of new HIV transmissions by at least 90 percent by 2030.
I believe that the EHE initiative and the national strategy provide a great road map for addressing HIV. My goal is to push CDC’s role in implementing the HIV strategy forward and tweak it so it is more operational for delivering HIV services and data to end the epidemic. To end the epidemic, we must have a clear focus on the STI and hepatitis syndemics and we must address the systemic racism, sexism, homophobia, and transphobia that hamper our progress. I’m thrilled that we are going to approach addressing HIV like a new outbreak all over again so we can end it.
Are there similarities or links in strategies to getting COVID and HIV under control?
Much of the infrastructure for COVID-19 is being built and utilized simultaneously. We need to ask questions about what assets from the COVID-19 infrastructure we could leverage for HIV and other health conditions once COVID-19 is under better control. For example, CDC has strongly encouraged the EHE jurisdictions to use novel and innovative activities to meet local needs in a tailored way, especially during COVID-19. Innovations in testing and care delivery spurred by COVID-19 could help us overcome longstanding barriers to HIV prevention and care in the long term by providing testing and care in more accessible, modern ways. These kinds of innovative approaches include the use or expansion of telemedicine and telehealth, rapid HIV self-tests, mail-in self-tests, and other locally tailored, creative solutions. It is also important to consider the lab and vaccine infrastructure being built for COVID-19 and how it can be leveraged for our other syndemics.
What are some things people living with HIV should know about the threat of not only COVID but also the isolation involved in lockdowns and the financial stress caused by the pandemic?
We are still learning about COVID-19 and how it affects people with HIV. Based on limited data, we believe people with HIV who are on effective HIV treatment have the same risk for COVID-19 as people who do not have HIV. However, the available data do indicate that people with HIV and serious underlying medical conditions might be at increased risk for severe illness. In some studies, people with HIV were also more likely to have these comorbidities than others with COVID-19 infection. Higher rates of COVID-related hospitalization, admission into intensive care units, and/or death among people with HIV seem to be driven by underlying conditions, lower CD4 cell count, and not being on effective HIV treatment.
During the COVID-19 pandemic, it is natural to feel stress, anxiety, and other emotions. Some healthy ways to cope with these feelings include taking breaks from the news, taking care of your body by eating right and getting at least eight hours of sleep, making time to do the activities you enjoy, and safely connecting with others to discuss your concerns and how you are feeling. If you have HIV and are taking your medicine, it is important to take everyday preventive actions, like wearing a mask, to prevent getting COVID-19; continue your HIV treatment; and follow the advice of your health care provider.
Tell us more about how your efforts in New York can succeed nationally.
I think that lessons I have learned both in my work in HIV in as well as my role as incident commander over the measles outbreak of 2019 and COVID-19 in New York City will be helpful to guide my work at DHAP on the national level. Listening more and talking less was an important part of my strategy in New York City and will be valuable in my new role at the CDC. Connecting to community, advocates, and my colleagues working on EHE will be a critical part of my new role. I am optimistic that my experience in New York City will be an important ingredient along with a healthy dose of humility and the voice of the national stakeholders in advancing my work at CDC.
Injectable HIV treatment has received Food and Drug Administration approval. Do you see that as an effective way to improve adherence for people living with HIV?
I think that the more options we have for treatment and prevention, the more likely individuals will be able to find an option that works in their lives. Similar to birth control, not every option is perfect for every person, nor is any one option the definitive solution to adherence problems. The amazing advances we are making in technology provide for a critical opportunity to implement multiple strategies at the same time with the goal of giving choices to an increasing number of people. Some people like pills. Some people will like shots. Some people will like implants. The more ways we have to deliver safe and effective medications, the more likely we are to find the right strategy for a larger number of people.
The concept of U=U (undetectable equals untransmittable) is becoming more widespread but isn't really part of the mainstream health conversation. How can we increase awareness of it?
U=U has been an important way to communicate that people with HIV on effective therapy with suppressed viral loads do not transmit the virus. I think that we need to continue to magnify the data to the community of providers that serve people with HIV as well as people who are otherwise affected. Working to create more status-neutral delivery of care regardless of HIV status is a way to bring the U=U message to life and address the institutions that maintain systems that support a divide between people with and without HIV. We have a way to go, but I am excited to work to further mainstream this important science.
Do you have any plans to battle HIV stigma as part of your position at the CDC?
Controlling the HIV epidemic means that we need to relentlessly address the root causes and social determinants that stand in our way. We need to aggressively work to disrupt the systems that create the schism between people based on their identity, including the result of their HIV test. Our work must challenge the core drivers of HIV, including stigma. This job is at its core is an opportunity to dismantle stigma, a challenge that has been key to my entire career.