Treatment
Many Living with HIV Have Limited Access to Food

Hidden beneath the shiny landscape of single-pill regimes and ever increasing lifespans, insufficient food access torments those living with HIV.
April 04 2018 8:00 AM EST
By continuing to use our site, you agree to our Privacy Policy and Terms of Use.
Hidden beneath the shiny landscape of single-pill regimes and ever increasing lifespans, insufficient food access torments those living with HIV.
Insufficient food access torments many of those living with HIV (and, for some, struggling with the complications of AIDS). Worse, for those those facing food insecurity, any assumption that HIV has become a manageable condition is rendered obsolete.
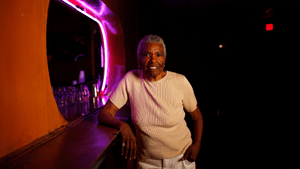
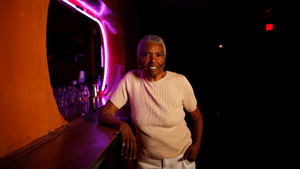
“You just have to find a way,” quotes David Brathwaite-Hill.
His apartment is cluttered, evidence of a lifetime spent in the East Village scattered between exposed brick walls. But the space is welcoming, pulling guests into a tender embrace. Although I have never been here before, the environment is somewhat familiar, comforting. A mocking nostalgia seeps forth, the soul pleading a return to a life yet lived under these worn wooden beams.
“How are you meant to ‘find a way?’” he laughs, recalling one provider’s worthless advice. Such had been the solution offered to his conundrum about how to consume healthy food on a limited budget. I lose him in thought, his fingers tugging on the nipple rings that dangle from his bare chest.
Since being diagnosed with HIV in 2013, Brathwaite-Hill, now 62, exists as yet another ignored statistic in the murky world of HIV and food insecurity. Too “rich” to qualify for SNAP (food stamps) and too poor to afford a healthy balanced diet, he lives week to week. This month, he is forgoing part of his treatment in order to buy nutrient-dense foods.
For people living with HIV, consuming nutritious foods and adhering to antiretroviral therapy work in symphony, fortifying and protecting the immune system. Often, for those of a lower socioeconomic status, a group disproportionately affected by HIV, this symphony shatters. Sacrifices are made, while immune systems are left vulnerable and exposed.
Food insecurity, be it chronic or intermittent, disrupts adherence to antiretroviral therapy. Taken in the absence of food, ART can upset the stomach. To avoid this, many people miss doses when food supplies dwindle. The hunger and stress associated with food insufficiency, also increases the probability of simply forgetting to take medication. Erratic adherence to ART is troubling. Drug resistance can develop, creating future treatment challenges. Studies also show that poor ART adherence allows viral loads to escalate and CD4 counts to plummet. A rep from the New York nonprofit God’s Love We Deliver notes that many of its HIV-positive clients facing food insecurity aren’t able to get their viral loads down to undetectable levels — which means they remain capable of transmitting HIV to others.
For those dealing with food insecurity, even perfect adherence to their drug regimen may be in vain. To reach full efficiency, certain drugs must be taken with food. The non-nucleoside reverse transcriptase inhibitor, rilpivirine, must be consumed with at least 500 calories, a challenging daily requirement for those with limited calorific access. The drug plasma concentration of atazanavir increases 70 percent when taken with a light meal. Ritonavir is equally dependent on food. In a sample of 400-plus food insecure HIV-positive individuals in Atlanta, Ga., researchers found that over half the participants were on meds that required food. Individuals on food-dependent ART regimes were also more likely to have to choose between the purchase of food or medication. Unsurprisingly, those on food-dependent regimes were significantly more likely to display lower CD4 counts and higher viral loads. This situation is unlikely unique to Atlanta. It is very likely happening all across America.
Food insecurity has no face. Unless an individual expresses difficulty in accessing food, it is nearly impossible for providers to make necessary medical adjustments. Confronting and admitting difficulties in food procurement is not easy. Many don’t recognize the importance of revealing their food insecurity when establishing ART. This is especially true for those experiencing intermittent insecurity. This will not last; this is just a phase; others are in greater need, they tell themselves.
Stigma and shame affect those living with both HIV and food insecurity. Eradicating this is paramount at the Keith Haring Food Pantry, one of the many services provided by New York City’s Gay Men’s Health Crisis. Situated above the streets of Manhattan, the room is hidden. There are no windows and no branded grocery bags. Individuals choose their food in near privacy, under the watchful care of a registered dietician. Canned foods and other non-perishables line the walls, while a large fridge offers fresh fruits and vegetables, organic where possible. Sadly, on this particular day, only bulbs of garlic remain for the taking.
Yet, there is a certain pride to be felt. That the Keith Haring Food Pantry even exists is reason for celebration. In 2016, GMHC served over 120,000 meals through both the pantry and its in-house meal program. Popular hands-on cooking classes are also offered, along with general nutrition and food safety training. Similarly, each client of God’s Love We Deliver completes a comprehensive nutrition assessment with one of seven registered dietitians. Advice on cooking with limited access and resources enables individuals to make informed decisions. In an insecure world, education fosters greater stability.
Despite the positive roles these organizations play, food insecurity remains a significant problem for people living with HIV, even in resource-rich locations. The Keith Haring Food Pantry has historic waitlists. Owing to the nature of the federal grants received by God’s Love We Deliver, clients are required to provide eligibility documents every six months. This creates challenges for those who struggle to constantly access updated records. As a result, delays in care and diet may result. A recent study in New York City found that out of 2,118 HIV-positive people receiving federal nutrition-based assistance, only 14 percent were constantly food sufficient. With ever-escalating food prices, the situation is only set to worsen.
Unfortunately, the current administration is showing no signs of increasing funding that’s so vitally needed. For now, all we can do is raise awareness. Recognizing the relationship between HIV and food insecurity should encourage individuals to seek culinary education. Understanding the importance of ART adherence and nutritional intake must foster dialogue between providers and clients, for it is the responsibility of both to ensure optimistic treatment outcomes. For instance, while ART may not feasibly be switched to less food-dependent regimes, specific nutritional care programs could be enforced for specific individuals. So long as we bring food access to the forefront of HIV discourse, we will begin to find ourselves in a far more optimistic position.